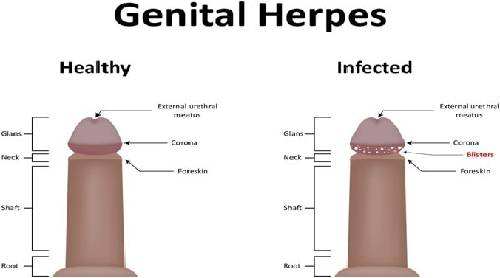
Genital herpes (GH) is a chronic sexually transmitted viral infection, characterized by asymptomatic viral shedding. In most cases, both primary infection and recurrences are asymptomatic. When symptomatic, primary GH may present with grouped vesicles at the site of inoculation associated with significant pain and regional lymphadenopathy. When aware of GH, individuals may notice mild symptoms, uncommonly of recurring outbreaks of vesicles at the same site. Most symptoms from GH relate to the psychological stigma of having a chronic transmissible STD. Neonates are susceptible to HSV infection when exposed perinatally, with risk of significant morbidity and mortality.
Causes of Herpes Simplex Virus: Genital Infections
HSV infection is transmitted through close contact with a person shedding virus at a peripheral site, mucosa surface, or secretion. HSV is inactivated promptly at room temperature; aerosol or fomitic spread unlikely. Infection occurs via inoculation onto susceptible mucosal surface or break in skin. Subsequent to primary infection at inoculation site, HSV ascends peripheral sensory nerves and enters sensory or autonomic nerve root ganglia, where latency is established. Latency can occur after both symptomatic and asymptomatic primary infection. Recrudescences may be clinically symptomatic or asymptomatic.
Symptoms of Herpes Simplex Virus: Genital Infections
Most people who are infected with HSV never develop any symptoms. When symptoms do occur, they vary widely from person to person. Symptoms of a first episode of genital herpes usually appear within two to 10 days of exposure to the virus and last an average of two to three weeks. Early symptoms can include:
- Itching or burning sensation.
- Pain in the legs, buttocks, or genital area.
- Vaginal discharge.
- Feeling of pressure in the abdominal region.
Diagnosis
Because in most cases intermittent asymptomatic shedding is occurring and lesions are “atypical” (not grouped vesicles on erythematous base), GH must be confirmed by viral culture or DFA.
Treatment
Topical Antiviral Therapy No significant efficacy.
Oral Antiviral Therapy Antiviral agents provide partial control of symptoms and signs of herpes episodes when used to treat first clinical episode or when used as suppressive therapy. They neither eradicate latent virus nor affect subsequent risk, frequency, or severity of recurrences after drug is discontinued. Even after laboratory testing, at least a quarter of patients with GH have no laboratory-confirmed diagnosis. Many experts recommend treatment for chancroid and syphilis as well as GH if the diagnosis is unclear or if the patient resides in a community in which chancroid is present.
- First clinical episode (primary or first symptomatic) Antiviral agents are more effective in treating primary infections than recurrences. Most effective when initiated ≤ 48 h after onset of symptoms.
- Acyclovir 400 mg tid or 200 mg 5 times daily for 7-10 days or until clinical resolution occurs.
Daily suppressive therapy Reduces frequency of recurrences by at least 75% among patients with frequent (more than 6-9 per year) recurrences. Suppressive treatment with oral acyclovir does not totally eliminate symptomatic or asymptomatic viral shedding or the potential for transmission. Safety and efficacy have been documented among persons receiving daily therapy for as long as 5 years. Acyclovir resistant strains of HSV have been isolated from some persons receiving suppressive therapy, but these strains have not been associated with treatment failure among immunocompetent patients. After 1 year of continuous therapy, acyclovir should be discontinued to allow assessment of the patient’s rate of recurrent episodes.
Prevention of GH
Sexual transmission
- Patients should be advised to abstain from sexual activity while lesions are present.
- Use of condoms should be encouraged during all sexual exposures.
- Efficacy of chronic suppressive therapy not proven.
- Patients with GH should be told about the natural history of the disease, with emphasis on the potential of recurrent episodes, asymptomatic viral shedding, and sexual transmission.
- Sexual transmission of HSV has been documented to occur during periods without evidence of lesions. In discordant couples, transmission usually occurs during period of asymptomatic shedding.
- Risk for neonatal infection should be explained to all patientsmale and female-with GH.
Perinatal transmission
Many experts recommend serotesting for HSV-1 and HSV-2 (Western blot) at the first prenatal visit. Infants born to women who asymptomatically shed HSV have reduced birth weight and increased prematurity.
References
- https://www.cdc.gov/std/tg2015/herpes.htm
- http://www.who.int/news-room/fact-sheets/detail/herpes-simplex-virus
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2564733/