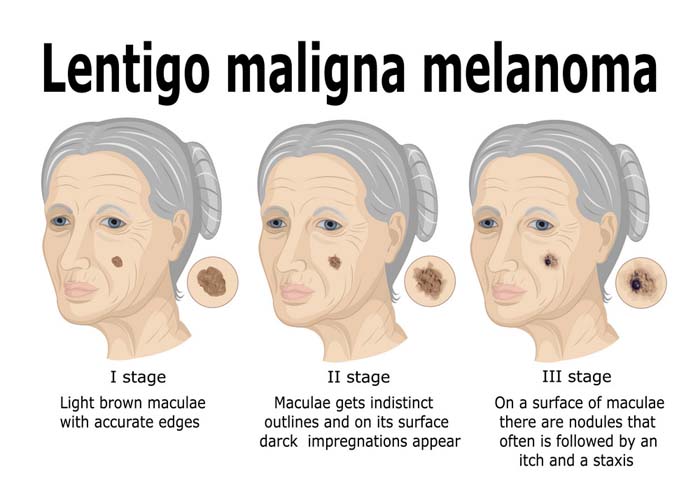
Lentigo maligna melanoma is the least common (<5%) of the three principal melanomas of white persons [superficial spreading melanoma (SSM), nodular melanoma (NM), and lentigo maligna melanoma (LMM)] and occurs in older persons on the most sun-exposed areas, the face and forearms. Although there is still some debate about the role of sunlight in the pathogenesis of malignant melanoma, few question the role of sunlight in the pathogenesis of LMM; the tumor was first noted on the faces of women working outdoors in the vineyards of France by Dubreuilh, who called it melanosis circumscripta praeblastomatosa. Lentigo maligna (LM) is a flat (macular) intraepidermal neoplasm and a melanoma in situ. It is the precursor or evolving lesion of LMM. Focal papular and nodular areas signal invasion into the dermis; the lesion is then called LMM.
Causes of Lentigo Maligna and Lentigo Maligna Melanoma
In contrast to SSM and NM, which appear to be related to intermittent high-intensity sun exposure and occur on the intermittently exposed areas (back and legs) of young or middle-aged adults, LM and LMM occur on the face, neck, and dorsa of the forearms or hands; furthermore, LM and LMM occur almost always in older persons with evidence of heavily sun-damaged skin (telangiectasia, marked freckling, atrophy, solar keratosis, basal cell carcinoma).
Symptoms of Lentigo Maligna and Lentigo Maligna Melanoma
Symptoms of lentigo maligna are lesions on the skin that appear tan to brown and occur on the head, neck and back of the hands. They are typically two to six centimeters in length and are irregularly shaped with darker spots.
Diagnosis
Lentigo maligna can be confused with lentigo benigna or simplex because elderly people commonly develop brown patches on the face secondary to actinic damage and only in a few cases they are lentigo maligna. Some lentigines have associated systemic disorders along with the skin lesions. Lentigenes frequently may be diagnosed through an incisional shave biopsy, submitted to a qualified dermatopathologist alongside with the corresponding clinical history to establish whether t
Treatment
- Excise with 1-cm or greater margin beyond the clinically visible lesion, provided the flat component does not involve a major organ. Use of Wood’s lamp helps in defining borders. ≥ 2 mm tumor thickness excise with 2 cm margin.
- Excise down to the fascia. Graft may be needed. Margin width > 1 cm is determined by location; a greater margin should be obtained if technically possible.
- No node dissection recommended unless nodes are clinically palpable. Sentinel node to be done in lesions > 1.5 mm in terms of thickness.
References