

Approximately 600,000 new infections with Neisseria gonorrhoeae occur each year. Most infections among men produce symptoms that cause them to seek curative treatment soon enough to prevent serious sequelae-but this may not be soon enough to prevent transmission to others. Many infections among women do not produce recognizable symptoms until complications [e.g., pelvic inflammatory disease (PID)] have occurred. In males, the most common presentation is an acute urethritis; in females, cervicitis. Others sites in the genitourinary tract may become infected as well as the rectum, pharynx, and conjunctiva. Both symptomatic and asymptomatic cases of PID can result in tubal scarring that leads to infertility or ectopic pregnancy. Because gonococcal infections among women are often asymptomatic, an important component of gonorrhea control continues to be the screening of women at high risk for STDs. Gonococcemia results in seeding of multiple sites, most commonly the joints and skin, resulting in disseminated gonococcal infection (DGl).
Causes of Neisseria Gonorrhoeae Infections
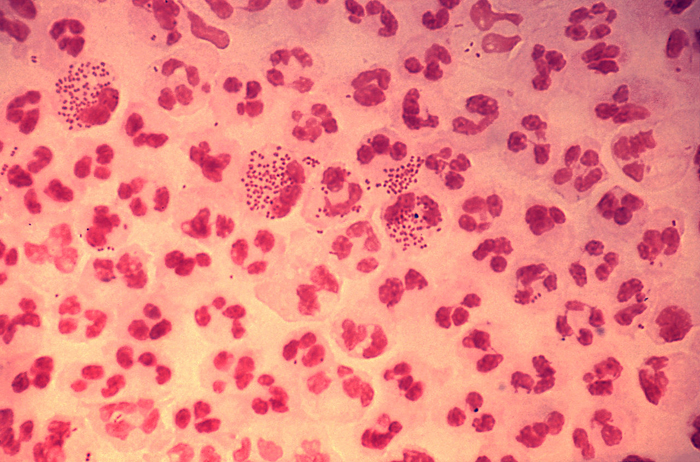
Gonococcus has affinity for columnar epithelium, while stratified and squamous epithelia are more resistant to attack. Epithelium is penetrated between epithelial cells, causing a submucosal inflammation with PMN reaction with resultant purulent discharge. Strains of gonococcus that cause DGI tend to cause little genital inflammation and thereby escape detection. These strains have become uncommon in the United States during the past decade. Most signs and symptoms of DGI are manifestations of immune-complex formation and deposition. Multiple episodes of DGI may be associated with abnormality of terminal complement component factors.
Symptoms of Neisseria Gonorrhoeae Infections
Symptoms include a purulent (or pus-like) discharge from the genitals which may be foul smelling, a burning sensation during urination and conjunctivitis commonly in neonatal infection, also occasionally in adults.
Treatment
Antimicrobial regimens Most patients with incubating syphilis may be cured by any of the regimens containing ceftriaxone or doxycycline. There is a high frequency of chlamydial infections in persons with gonorrhea, and treatment regimens cover this possibility.
Follow-up Persons with uncomplicated gonorrhea who are cured with any of the preceding regimens need not return for test-of-cure. Persons with persisting symptoms after treatment should be evaluated by culture for N. gonorrhoeae, and any gonococci isolated should be evaluated for antimicrobial susceptibility. Infections detected after treatment with one of the recommended regimens more commonly occur because of reinfection rather than treatment failure, indicating a need for improving sex partner referral and patient education. Persistent urethritis, cervicitis, or proctitis also may be caused by C. trachomatis and other organisms.
Management of sex partners Sex partners should be referred for evaluation and treatment. Gonococcal infection is often asymptomatic in sex partners of patients with DGI. As for uncomplicated infections, patients should be instructed to refer sex partner(s) for evaluation and treatment.
Prevention
Use of condoms should be encouraged.
References

