Pityriasis versicolor (PV) is a chronic asymptomatic scaling dermatosis associated with the superficial overgrowth of the hyphal form of Pityrosporum ovale, characterized by well-demarcated scaling patches with variable pigmentation, occurring most commonly on the trunk.
It sometimes called ‘tinea versicolor’, although the term ‘tinea’ should strictly refer to infection with a dermatophyte fungus.
Causes of Pityriasis Versicolor
Dicarboxylic acids formed by enzymatic oxidation of fatty acids in skin surface lipids inhibit tyrosinase in epidermal melanocytes and thereby lead to hypomelanosis. The enzyme is present in the organism.
Symptoms of Pityriasis Versicolor
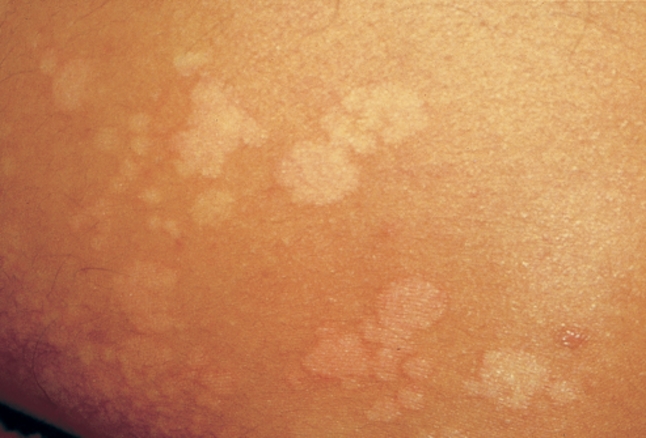
Pityriasis versicolor is commonly seen on the upper part of the back and on the chest, but it can be found on the entire body.
In the summer the infection is seen as well-defined, uneven patches. The patches are pale-red or brownish, and scaly. The patches often merge into big blotches that may look like maps. Sunbathing evens out the colour and makes the condition less visible.
In the winter the patches become scaly and change colour. In people who have tanned skin, this stage is quite visible as these patches appear white. It is at this point that most people first consult their doctor.
Diagnosis
Clinical findings, confirmed by positive KOH preparation findings.
Scrapings of the skin may be sent to the laboratory to check for the fungus. More simply, shining an ultraviolet light onto the rash will make the patches fluoresce a yellow green colour (this is known as a Wood’s Light test).
Treatment
Topical agents
- Selenium sulfide (2.5%) lotion or shampoo: Apply daily to affected areas for 10 to 15 min, followed by shower, for 1 week
- Propylene glycol 50% solution (in water): Apply bid for 2 weeks
Systemic therapy (None of these agents is approved for use in PV in the United States).
- Ketoconazole 200 mg/d PO for 7-14 days or 400 mg once; repeat in 1 week or 400 mg stat, repeat in 1 month
- Fluconazole 400-600 mg stat; repeat in 1 week
Secondary prophylaxis Ketoconazole shampoo once or twice a week. Selenium sulfide (2.5%) lotion or shampoo. Salicylic acid/sulfur bar. Pyrithione zinc (bar or shampoo). Propylene glycol 50% solution once a month.
References